Outreach program decreases health care resource use among children with asthma
January 19, 2024
6 min read
Add topic to email alerts
Receive an email when new articles are posted on
Please provide your email address to receive an email when new articles are posted on .
”
data-action=”subscribe”>
Subscribe
We were unable to process your request. Please try again later. If you continue to have this issue please contact [email protected].
Back to Healio
Key takeaways:
- Access to care, fragmented care, insufficient asthma education and social determinants of health impact asthma outcomes.
- A comprehensive team engages patients and addresses each of these barriers.
A community outreach program decreased health care resource use among children with high-risk asthma in Tennessee by targeting specific barriers to care, according to a report published in Annals of Allergy, Asthma & Immunology.
Patients who participated in the program experienced these improvements within a year of enrollment, Christie F. Michael, MD, associate professor in the department of pediatrics at The University of Tennessee Health Science Center, and colleagues wrote in the report.
Data were derived from Steppe S, et al. Ann Allergy Asthma Immunol. 2023;doi:10.1016/j.anai.2023.12.002.
Statewide data indicated an annual average of 1,042 ED visits and 96 hospitalizations for asthma per 100,000 individuals in Tennessee between 2012 and 2016. In metro Shelby County, which includes Memphis, averages included 1,996 ED visits and 165 hospitalizations per 100,000 individuals.
“Shelby County has the highest-risk asthma population in the state despite not having the highest asthma prevalence in Tennessee,” Michael told Healio.
The Changing High-Risk Asthma in Memphis through Partnership (CHAMP) program, of which Michael is the medical director, was designed to combat the barriers that contribute to these high rates, including lack of access to care, fragmented care, insufficient asthma education and social needs and social determinants of health.
Implemented solutions
Michael said there are many reasons why Shelby County has increased risks for asthma, including reasons related to human nature and the tendency to consider asthma an acute problem instead of a chronic one.
“However, the fact that Medicare-insured patients visit the hospital and emergency room twice as often as privately insured in Shelby County suggests that these health disparities could be addressed at least in part by addressing social determinants of health,” Michael said.
“Because of our community connection and presence in the home, we have learned many things about patients and families that help us better support them,” she continued.
The program has cared for families who have been homeless and living in abandoned buildings or cars, Michael said. Also, many families have experienced difficulties as renters and have needed legal support to address issues such as leaking roofs.
“Food insecurity and transportation issues are common,” Michael continued, adding that childhood experiences such as violence and abuse impact quality of life as well.
“We focus on building relationships which foster trust,” she said. “We all benefit from that. Every member of our leaderful team is passionate about improving the lives of our patients.”
To ensure access to care, CHAMP developed a dedicated medical team, established a 24-hour call line and a sick-call triage, and provided transportation services. The members of the medical team can be reached via cell phone during business hours as well.
“If we want patients to do something other than wait until they are sick and visit the ED, we must give them options and be more accessible,” Michael said.
The program also aimed to have patients see the same providers at each visit. After visits, members of the team follow up with patients to monitor their status and arrange additional care.
Noting that care often requires multiple providers in different locations, leading to fragmented care, CHAMP also created an asthma data repository that includes information about the team’s activities and claims data from the state’s Medicaid program, TennCare, in addition to data from electronic medical records.
Community health educators and members of the medical team identify and address deficits in education about subjects such as medication adherence and inhaler technique via conversations with patients and caregivers, and these messages are reinforced during office and home visits as well as at school.
“CHAMP is designed to break down the walls of the clinic and extend into the community where children live and attend school,” Michael said. “We coordinate with school nursing and provided in-service asthma education to school nurses annually.”
Also, nearly all the children in the program are from households with only one caregiver that fall below poverty guidelines and are characterized by environmental hazards that exacerbate asthma episodes.
CHAMP partners with families, primary care providers, medical-legal services and community programs or services such as Habitat for Humanity to address these environmental triggers.
Eligibility includes Shelby County residents aged 2 to 18 years enrolled in Medicaid or TennCare with three or more asthma-related ED or urgent care visits during the previous year, two or more hospitalizations related to asthma in the previous year, or at least one ICU admission in the prior 2 years.
Physicians also may admit patients who are on the cusp or eligibility criteria or who have special circumstances at their discretion. Typically, about 30% of eligible patients complete enrollment in the program.
Results
CHAMP enrolled 1,348 children between January 2013 and December 2022, and 945 (63% boys; 90% Black; mean age at enrollment, 6.8 years) completed a full year.
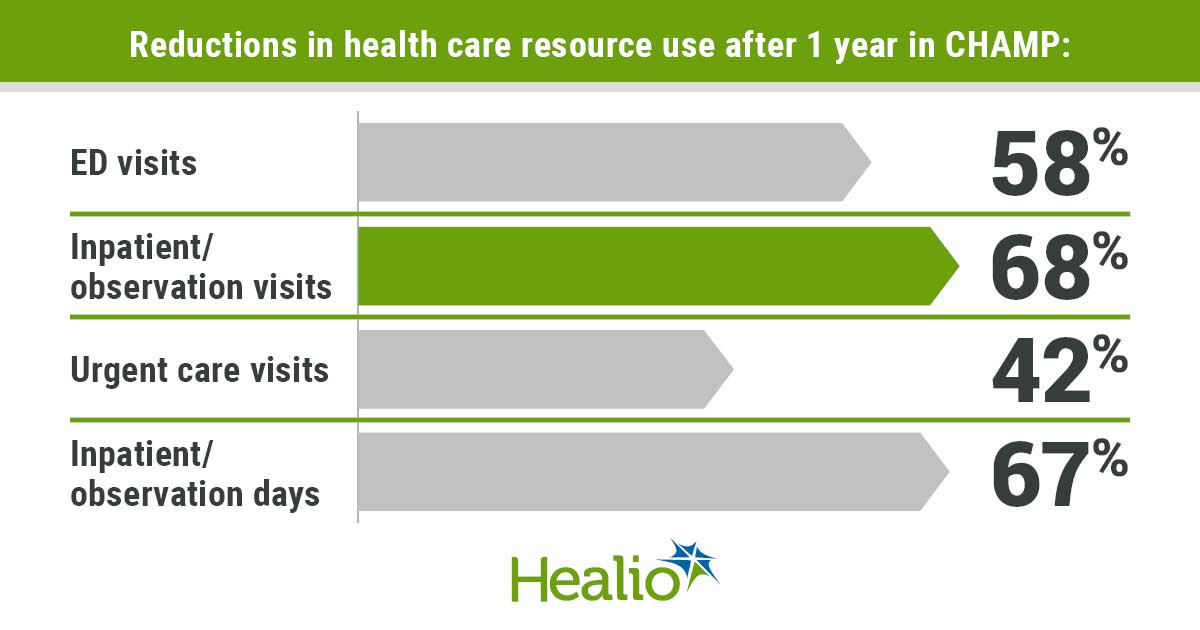
Compared with the year before these patients enrolled in CHAMP, ED visits fell by 58%, inpatient and observation visits declined by 68%, and urgent care visits dropped by 42% after a year in the program.
Also, these patients experienced a 67% decrease in inpatient and observation days and a 95% decrease in regular outpatient clinic visits, in addition to a 53% drop in total number of asthma exacerbations. Per patient, the number of exacerbations fell from 2.97 to 1.4.
The authors called the decreases per patient in health resource utilization outcomes including ED, inpatient, urgent care and sick outpatient visits after a year of participating in the program significant.
Between November 2013 and December 2022, there were 1,053 calls from the families of 415 unique participants to the 24-hour call line, including 58% calls after hours, or between 5:01 p.m. and 7:59 a.m.
About half (52%) only called the line once. Two-thirds (67%) were classified as related to an immediate breathing issue related to asthma, and 19% were from patients who needed a prescription. Also, 52% of these issues resolved without any visit to a medical facility.
Compared with a statewide matched control group of children with asthma in TennCare, a 3-year, third-party evaluation published in 2017 found that CHAMP reduced costs by $545 per child per quarter, or $2,180 per year.
CHAMP also improved quality of life for these families, Tonya Winders, MBA, study coauthor and president of Global Allergy & Airways Patient Platform, told Healio.
“The CHAMP program not only positively impacted the children enrolled and directly impacted, but also the caregivers,” Winders said.
CHAMP’s timely and tailored approach addressed the basics of good asthma care while empowering the families by establishing trust and developing self-management skills vital to managing chronic diseases, she continued.
“Most participants reported feeling heard and valued like never before by the health system,” she said.
Next steps
The authors attributed CHAMP’s success to its ability to find and engage patients in a timely manner and its implementation of the call and triage lines. Also, the data repository facilitated care coordination between the medical and community teams despite challenges in maintaining it.
“We had one that housed all the community activity and the claims data from insurance, but this has not been supported by the institution for some time,” Michael said.
Also, the two repositories that have since been added to the system have not been as effective as the first. Both require extensive labor for transferring claims data from TennCare as well.
“This information should be readily available to providers in order to optimize patient management,” Michael said.
The community health educators also were cited for their work.
Despite these successes, the authors noted that only 30% of eligible patients participate. Obstacles to greater participation include patients who do not answer the phone or provide accurate contact information. Also, the authors said that caregivers often say they are not interested, they do not have time, or they mistrust home visits.
Additional challenges included the establishment of the various roles in the program, along with managing staff and system changes including changes to electronic medical records, TennCare claims data systems and data transfers.
Financial sustainability is difficult too, the authors continued. CHAMP’s initial funding came from a 2012 Centers for Medicare and Medicaid innovation award. It is now funded mostly by institutional support with additional reimbursement from two of TennCare’s three branches.
“We have created a program that has been successful in reducing ED visits, urgent care visits and hospitalizations for over 10 years,” Michael said. “Yet we have had to fight daily to maintain operation.”
The authors said the best opportunities for sustainable funding lie with contractual relationships with payers and that they are working to establish these relationships.
As the program is ongoing, the authors continued, scaling the program to achieve these outcomes for the largest number of patients is key to sustainability as well.
Michael also offered advice for other health care systems that may want to replicate CHAMP’s success.
“Ask the views of the providers who see the most asthma in your community and include them in decision-making,” she recommended.
Also, Michael urged other programs to request access to claims data such as encounters and medications from involved payers.
“Use statewide data regarding asthma and compare your county to others to determine distinctions,” she said.
Finally, she said, other programs should address social determinants of health, such as by determining what the other available health care options are in the underserved community, specific to their populations.
“We firmly believe the success of CHAMP is related to a dedicated community and medical team that collaborate to provide extra services that are not reimbursed in the current system,” Michael said.
“Publication of this paper describing the CHAMP program should help garner more support and leverage this successful innovation to affect changes in reimbursement that could make programs like CHAMP sustainable,” she said.
For more information:
Christie F. Michael, MD, can be reached at [email protected]. Tonya Winders, MBA, can be reached at [email protected].
Sources/Disclosures
Collapse
Disclosures:
Michael reports no relevant financial disclosures. Winders reports employment as president of Global Allergy & Airways Patient Platform. The other authors report no relevant financial disclosures.
Add topic to email alerts
Receive an email when new articles are posted on
Please provide your email address to receive an email when new articles are posted on .
”
data-action=”subscribe”>
Subscribe
We were unable to process your request. Please try again later. If you continue to have this issue please contact [email protected].
Back to Healio