
Neurological
Does Increased Cardiorespiratory Fitness Decrease Alzheimer’s Risk? The Impact of Physical Fitness on Neurodegeneration

Dementia is a worldwide public health concern. There are 35.6 million people worldwide with dementia; by 2030, estimates are that 75.6 million people worldwide will have dementia. Dementia prevalence doubles every 5 years after age 65, and by age 90, nearly 1 in 3 adults will meet the diagnostic criteria for dementia.1
Hallmarks of aging include chronic low-grade inflammation, mitochondrial dysfunction, and neurodegenerative changes. The concept of “inflammaging,” introduced in 2000 by Claudio Franceschi, correlates aging with elevated inflammatory markers, which make older individuals more susceptible to chronic morbidities, including Alzheimer disease (AD).2 Oxidative stress and mitochondrial dysfunction in AD perpetuate an imbalance in neuronal cell function, generating further malfunction. In AD, brain atrophy and reduction in cerebral perfusion are significant, with a yearly hippocampal volume reduction of 3.5% in people with mild cognitive impairment compared with 1% to 2% in healthy controls aged 55 and older.3,4 Cerebral blood flow is decreased up to 40% in patients with AD compared to healthy controls.5
Cardiorespiratory fitness, as measure by VO2max (volume of oxygen per kilo of body weight per minute) is affected by age, gender, genetics, exercise type, and training intensity. After age 20, it is estimated that VO2max decreases by 3% to 6% each decade, with a jump to more than 20% decline per decade after age 70.6 Several studies correlate higher VO2max with lower inflammation, reduced oxidative stress, improved mitochondrial function, and improvement in brain structure and functional connectivity.5,6,7
Effective treatments for Alzheimer disease (AD) are lacking, which is shifting the focus to disease prevention. While the benefits of exercise are frequently noted, reported measurements of physical fitness are inconsistent across studies, and many participants self-report their physical activity. Recommended guidelines for exercise are also vague. Considering the effects of cardiorespiratory fitness on inflammation, mitochondrial structure, and cerebral anatomical changes will aid in providing future recommendations for dementia prevention, including AD, and overall cognitive health.
Cellular Aging and Inflammation as a Cause of Dementia
A number of cellular changes are associated with chronic low-grade inflammation and impairment in immune function. Shrinking of the thymus is one of the most dramatic changes that occurs in an aging immune system. Naïve T-cells leave the thymus to circulate in the blood and lymphatic system to protect against pathogens. Memory T-cells form after antigen exposure. With age, T-cells develop underlying defects and decline in activity, contributing to chronic inflammation and decreased immunity. Naïve T-cell production (CD4 and CD8) also declines with age, and memory T-cell production increases. In older individuals, memory CD4 T-cells show impaired mitochondrial function and increased production of reactive oxygen species.8 During chronic inflammation associated with age, pro-inflammatory cytokines, such as interleukin (IL)-6, tumor necrosis factor (TNF), and IL-1β, cross the blood-brain barrier, triggering microglia and astrocytes to produce pro-inflammatory cytokines over anti-inflammatory cytokines.9
Increased dementia risk is noted with comorbid neuropsychiatric and cardiovascular conditions and high systemic inflammation. Apolipoprotein E gene variant APOEε4 is the strongest genetic risk factor for dementia. APOEε4 is also linked to atherosclerosis and the modulation of inflammatory cytokines through promoting innate immune response.10 Beeri et al noted that having 2 or more cardiovascular risk factors in midlife predicted an increase in amyloid aggregation later in life.11 The researchers noted that midlife risk factors outweigh late-life risk factors in the development of dementia. Gottesman et al found that 2 or more cardiovascular risk factors (BMI ≥30, smoking, hypertension, diabetes, hypercholesterolemia) in midlife had an odds ratio of 2.88 for later-life brain amyloid deposition.12 This is important to note since the neurodegenerative changes of dementia begin decades before clinical symptoms are evident.
Neuroinflammation is evident in the progression of AD through increasing amyloid plaques and neurofibrillary tangles (NFTs).13 Overactivation of the immune response is more pronounced in AD because of the accumulation of amyloid β protein (Aβ).5 So-called proteinopathies, which occur due to misfolding of toxic proteins, produce extracellular Aβ plaques and intracellular NFTs. When amyloid beta precursor protein (APP) is cleaved by gamma-secretase, an Aβ-peptide forms containing 42 amino acids, known as Aβ42, which is the most toxic variant.9 In addition to tau and phosphor-tau, Aβ42 is a biomarker for AD that can be measured in cerebrospinal fluid via lumbar puncture.9 The accumulation of pathologic Aβ42 in the AD brain is attributed in part to impaired mitophagy.14
The presence of Aβ plaques contributes to the hyperphosphorylation of tau. The functioning of tau, the major microtubule-associated protein in neurons, is regulated by its degree of phosphorylation. Increased tau phosphorylation decreases microtubule stability and is correlated with neurotoxicity. In AD, tau is noted to be 3 to 4 times more phosphorylated, accounting for the increased formation of NFTs.14
In aging, prolonged immune activation causes impairment of phagocytosis by microglia and degradation of astrocytes.5 An essential role for microglia and macrophages in the central nervous system is to discard cellular debris, while astrocytes aid neuronal stability by modulating the blood-brain barrier.5 The phagocytic role of microglia in the central nervous system to degrade Aβ is compromised, which leads to the release of pro-inflammatory products. As a result, inflammatory cytokines, including ILIβ and TNF-α, pass the blood-brain barrier. Proinflammatory production of cytokines, reactive oxygen, and reactive nitrogen species furthers the production of Aβ and tau hyperphosphorylation through a positive feedback loop leading to more toxicity, as shown in Figure 1.5
Figure 1. Progression of amyloid β protein causes microglia inefficiency, and produces pro-inflammatory species (cytokines, reactive oxygen species [ROS], reactive nitrogen species [RNS]), causing further amyloid β production, and tau hyperphosphorylation, ultimately leading to neurodegeneration and cell death.
Effects of Exercise on Inflammation
Over the past 3 decades, several studies have correlated decreased inflammation with decreased AD risk. The Baltimore Longitudinal Study of Aging showed a 60% reduction in dementia in patients using NSAIDs for over 2 years. Zhang et al found a 19% risk reduction in AD with NSAID use from 16 cohort studies.15
Lack of physical activity is associated with elevated inflammatory biomarkers. For example, abdominal adipose tissue secretes TNF-α and other inflammatory markers.16 Conversely, physical activity increases hormones with immunomodulatory effects, increases anti-inflammatory myokines, decreases visceral fat, and decreases expression of toll-like receptors in immune cells.17 Exercise enhances immunocompetence by circulating immune cells to peripheral tissue. A study by Lavin et al showed that lifelong exercisers had significantly lower levels of IL-6 and higher levels of anti-inflammatory markers IL-10, TNF-α, TNF-β, and EP4.18 Repeated moderate intensity exercise is shown to have antioxidative effects, decrease oxidative stress, improve mitochondrial efficiency, and improve the immune function response.18 All of these factors result in a cumulative reduction in inflammation.
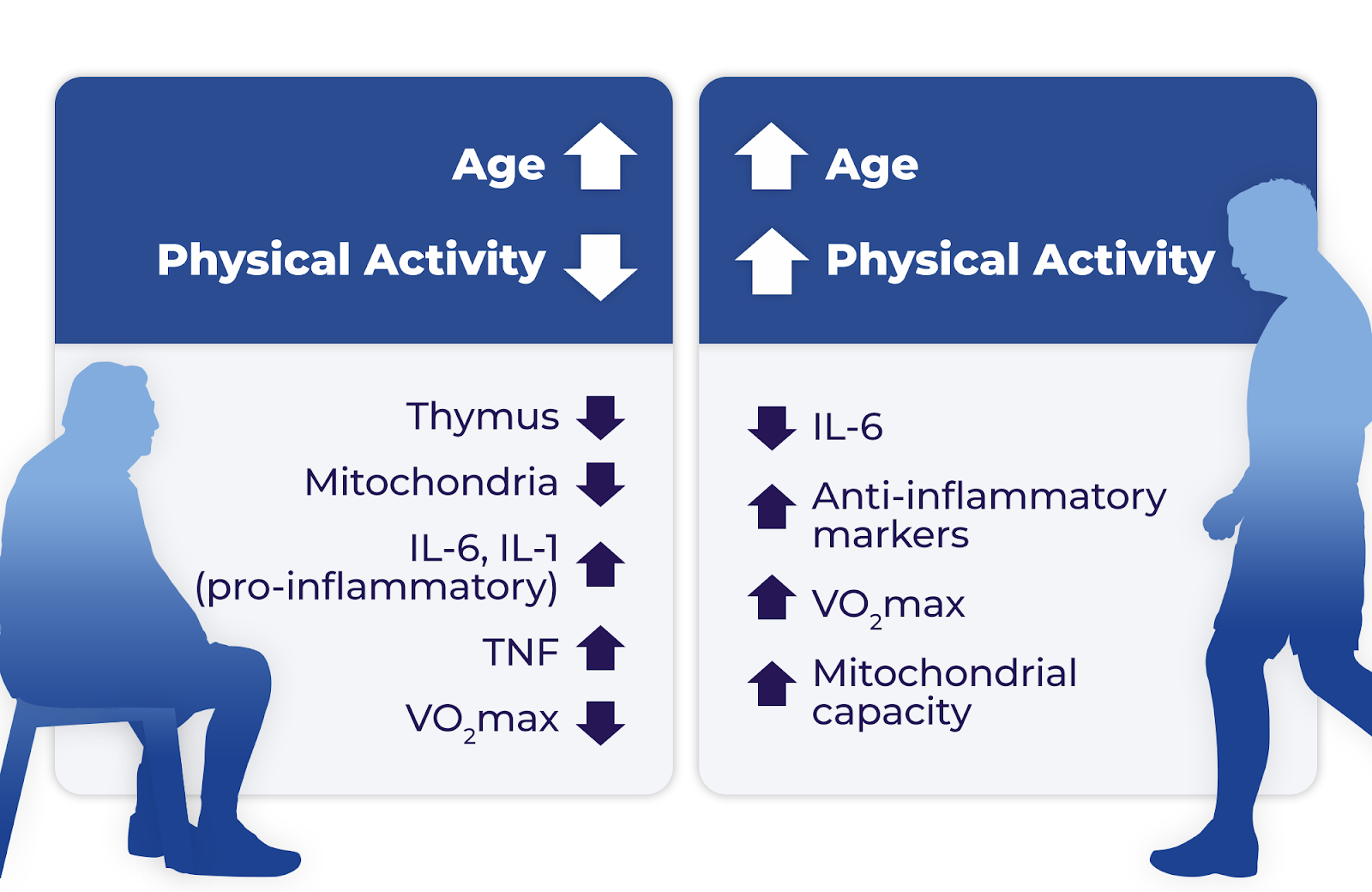
Dougherty et al studied 86 older adults at risk for AD, comparing cardiorespiratory fitness, hippocampal volume measured by magnetic resonance imaging (MRI), and memory measured by Rey Auditory Verbal Learning Test (RAVLT).19 The results differed based on gender, showing that VO2max was associated with increased hippocampal volume in women and improved RAVLT memory scores in men. Increased age and decreased physical activity correlate with impaired thymus function, impaired mitochondrial function, decreased VO2max, and increased inflammatory markers IL-6 and IL-1. An increase in physical activity in advancing age is associated with a reduction in IL-6 and increases in anti-inflammatory markers, VO2max, and mitochondrial capacity (Figure 2).19
Effects of Exercise on Mitochondrial Function
Mitochondria generates adenosine triphosphate (ATP) through oxidative phosphorylation. Additionally, calcium homeostasis, apoptosis, and reactive oxygen species (ROS) production are mitochondrial functions. The accumulation of amyloid β peptide within mitochondria is associated with the progression of AD; study findings show amyloid-β protein precursor and Aβ in mitochondria in AD patients before the formation of senile plaques.20
Mitochondria use oxygen to produce energy during metabolism. If ROS levels are unusually elevated, neurodegeneration occurs through the oxidation of proteins that causes damage to their structure. The ROS levels are regulated by mitophagy, a process by which damaged organelles are engulfed by vesicles and degraded by specialized proteins. With aging, the decreased efficiency of antioxidants and the increase in ROS cause toxicity, leading to cellular dysfunction and apoptosis.21
Postmortem brain studies of individuals with AD show that mitochondrial dysfunction occurs early in the disease process and is especially pronounced in the entorhinal-hippocampal system located in the medial temporal lobe. Cortical neurons in the entorhinal-hippocampal system layer II are thought to be where initial AD pathology occurs.14 Postmortem studies have also shown a decrease in the number and quality of mitochondrial DNA (mtDNA).20
Mitochondrial biogenesis, the creation of new, functioning mitochondria, is thought to be facilitated by physical activity.22 In 1965, the research of John O. Holloszy, MD, showed that endurance exercise training resulted in the doubling of mitochondria in rodent skeletal muscle. Endurance exercise training improves mitochondrial capacity, which enables protective antioxidant effects.22 He noted that mitochondrial biogenesis occurs with repeated bouts of exercise at sufficient intensities over a period of time.
Ding et al reported that regular exercise caused increased mitochondrial tricarboxylic acid enzymes and the synthesis of neurotrophins, including brain-derived neurotrophic factor (BDNF).23 BDNF is a mediator in PGC-1α-induced mitochondrial biogenesis and regulates antioxidant enzymes that reduce ROS seen in AD. A positive correlation between mitochondrial volume and VO2max has been noted since the 1970s.24 While VO2max is typically used to measure cardiorespiratory fitness, it depends on mitochondrial efficiency.23 In addition to mitochondria volume, endurance exercise and higher VO2max are associated with improvement in mitochondria respiratory function and oxidative capacity.24
More recent research has replicated the effect of exercise on mitochondria in other organs, notably the brain. The brain utilizes 20% of the body’s total oxygen and depends on mitochondria for 90% of its ATP production.20 Radak et al reported that endurance exercise increases VO2max and is associated with mitochondrial biogenesis partly through sirtuins (SIRT-3), a mitochondrial protein. SIRT-3 is responsible for oxidative phosphorylation, oxidation of fatty acids, and synthesis of ketone bodies. Endurance exercise increases SIRT-3 levels in the hippocampus, skeletal muscle, liver, and heart.25
Effects of Exercise on Brain Structure and Cerebral Blood Flow
General cerebral atrophy is a well-known occurrence with aging, and hallmarks of this include volume loss, cortical thinning, enlarged ventricles, and brain folding changes. Global volume changes begin at age 35 with a total brain volume loss yearly of 0.2%, which escalates to 0.5% annually after age 60.26 The hippocampus and prefrontal cortex appear more vulnerable to aging; the hippocampus and prefrontal cortex atrophy by 1% to 2% for every year after age 55.3 Cortical thinning occurs at a rate of 0.004 mm/year and is associated with memory decline. Ventricular enlargement occurs from the accumulation of cerebrospinal fluid in the ventricles, which causes compression of brain parenchyma. Specifically, the lateral and third ventricles are associated with impaired attention, visual memory, and speed.26 A study comparing middle-aged adults with healthy older individuals noted that sulci were, on average, 17.3% wider in elderly patients (aged 66-90 years).26 Of note, the most significant difference between the middle age and elderly adults was in the depth of the left superior frontal sulcus.26 A larger longitudinal study with 132 participants followed over a 7 year period found the largest rate of increase in fold opening in the superior frontal sulcus (0.131 mm/year). Like other neurodegenerative diseases, AD accelerates and intensifies structural changes that occur with aging.26
Vascular changes that occur with age include arterial stiffness, reduced capillary density, and increased blood-brain barrier permeability.26 Decreased cerebral blood flow is associated with increased dementia risk, and is noted prior to structural brain changes in AD. Reduced cerebral blood flow has been predictive of progression to AD from healthy controls and individuals with mild cognitive impairment.27
Exercise is correlated with increased hippocampal volume, hippocampal neuroplasticity28, increased gray matter volume28, white matter integrity3,, and cortical thickness.24 A 1-year study of 120 participants aged 55 to 80 found that moderate-intensity aerobic training showed a 2% increase in anterior hippocampal volume.29 Conversely, a study by Pani et al showed increased hippocampal atrophy in high-intensity interval training groups, and that brain structure was best preserved in those following the national guidelines of 30 minutes of physical activity per day. This study also noted that those with higher VO2max at inclusion had better-preserved brain structure.30 A study of 29 participants with mild cognitive impairment by Eisenstein et al correlated increased VO2max with reduced hippocampal volume. However, there was a decreased correlation between hippocampal volume and memory performance compared with low VO2max.4 Alfini et al determined that cessation of exercise for 10 days reduced hippocampal blood flow.7
Regular exercise and a higher VO2max in mid-life seem to have the most robust evidence for ameliorating cognitive changes that occur with age. A study by Kurl et al followed over 2000 men over 20 years and found that one standard-deviation increase in VO2max (3.5 mL/kg/min) correlated with a 20% decrease in dementia.29 Men with a VO2max less than 23.7 mL/kg/min (low cardiac fitness) had a 1.92-fold risk of developing dementia compared with those with a VO2max greater than 36.5 mL/kg/min at baseline testing.29 Horder et al followed 1462 women and reported a 9.5-year delay in dementia onset in more fit women in midlife.30
While these studies looked at how various exercise regimes influence VO2max, brain structure, and cognition, the most beneficial exercise program seems to be moderate-intensity cardiovascular exercise, performed consistently 5 to 6 days a week, and starting by mid-life. VO2max improves with repeated sessions of physical activity of at least 30 minutes that elevates the heart rate, such as brisk walking, jogging, biking or hiking. Although some studies indicate cognitive gains with single bouts of exercise, longer term studies highlight the importance of cardiorespiratory fitness starting in mid-life. Higher V02max at age 50 correlates with delaying dementia onset by a decade.30 Midlife cardiovascular risk factors (including BMI ≥30, smoking, hypertension, diabetes, hypercholesterolemia) are associated with elevated dementia risk later in life.12 Since exercise is known to improve cardiovascular risk factors, it seems likely that it should also reduce dementia risk. More research is needed in this area and to evaluate the effects of other forms of exercise, such as weight training or yoga, on cognitive decline.
Conclusion
AD is typically an age-related disease occurring later in life, with an increased risk associated with cardiovascular disease, diabetes, and obesity. As people continue to live longer, and the age of the world’s population increases, dementia is also increasing.
Inflammation is a known by-product of aging and exercise reduces inflammation. While reports of the impact of exercise on memory are conflicting, most show at least modest improvement in one or more aspects of cognition. Studies have shown that as little as a single exercise session can cause changes in the body.
Measurement of cardiorespiratory fitness utilizing VO2max is a way to standardize studies of physical fitness. Limitations include self-reported exercise and a minimal number of participants. As more studies are done, specific recommendations for VO2max levels will help individuals quantify their fitness goals to maximize their cognitive health.
Cynthia Sieto, MSPAS, DMSc, graduated with her MSPAS from DeSales University in 2001 and her DMSc from Rocky Mountain University in 2023. She has specialized in psychiatry for 20 years and is currently employed by St. Luke’s University Health Network in Allentown, PA. To maximize her cardiorespiratory fitness, she completed the 2023 NYC marathon.
This article originally appeared on Clinical Advisor




