TB testing practices may miss high-risk groups
January 24, 2024
2 min read
Add topic to email alerts
Receive an email when new articles are posted on
Please provide your email address to receive an email when new articles are posted on .
”
data-action=”subscribe”>
Subscribe
We were unable to process your request. Please try again later. If you continue to have this issue please contact [email protected].
Back to Healio
Key takeaways:
- Factors associated with testing positive for LBTI and those associated with being tested in general varied.
- Researchers say this could lead to missing patients who may be at higher risk for LBTI.
Current practices for latent tuberculosis infection testing may be missing high-risk patients, according to a study assessing factors associated with testing and positivity, researchers said.
“In the U.S., more than 80% of active tuberculosis (TB) cases occur due to reactivation of latent tuberculosis infection (LTBI). Current screening guidelines recommend screening asymptomatic adults based on birth, travel, or residence in a TB-endemic country, immunosuppression, and close contact with active TB,” Jennifer Ku, PhD, MPH, postdoctoral research fellow at Kaiser Permanente Southern California Department of Research & Evaluation, told Healio. “However, these variables are not routinely collected as part of clinical care, and guideline implementation has been suboptimal.”

Ku JH, et al. Clin Infect Dis. 2024;doi:10.1093/cid/ciae015.

Jennifer Ku
According to Ku, many low-risk individuals continue to be tested as a requirement for employment, school-based policies or congregate settings, such as nursing homes.
“Therefore, testing efforts disproportionally reach populations with low risk of LTBI, while populations with the highest risk are undertested,” she said.
To examine factors associated with LTBI testing and LTBI positivity, Ku and colleagues conducted a study between Jan. 1, 2008, and Dec. 31, 2019, at Kaiser Permanente Southern California. The study included all patients aged 18 and older with no history of active TB.
Among more than 3.8 million adults, 706,367 (19%) were tested for LTBI, among whom 60,393 (9%) had one or more positive result. Among more than 1.2million people meeting one or more of the screening criteria for LTBI, 210,025 (17%) were tested for LTBI.
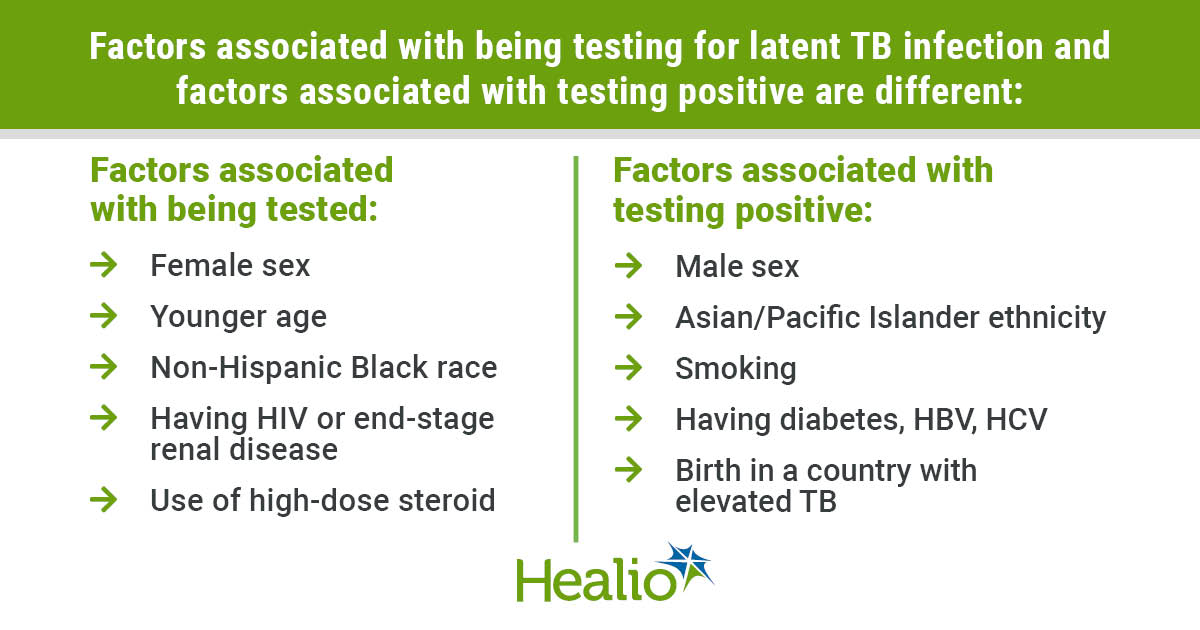
The researchers also found that factors most associated with testing positive for LTBI were not the same as the factors associated with LTBI testing.
For example, the study showed that factors associated with higher odds of testing positive included being male (adjusted OR = 1.32; 95% CI, 1.3-1.35), Asian/Pacific Islander (aOR = 2.78; 95% CI, 2.68-2.88), currently smoking (aOR = 1.24; 95% CI, 1.2-1.28), having diabetes (aOR = 1.13; 95% CI, 1.09-1.16), hepatitis B (aOR = 1.45; 95% CI, 1.34-1.57) or hepatitis C (aOR = 1.54; 95% CI, 1.44-1.66) and birth in a country with an elevated TB rate (aOR = 3.4; 95% CI, 3.31-3.49), none of which were associated with higher odds of LTBI testing.
Factors that did, however, increase odds for LTBI testing included being female, of younger age, non-Hispanic Black and specific immunocompromising conditions.
“Although some groups at high risk of LTBI are being appropriately tested, the current LTBI testing practice are still missing important high-risk groups,” Ku said. “Increasing testing in these high-risk individuals is a priority.”
She added that routine assessment for TB risk factors poorly documented in clinical practice (eg, place of birth, travel history) is needed moving forward, and that some important risk factors such as HBV and HCV, and race/ethnicity are readily available yet not considered in current screening guidelines.
“Additional work is needed to refine guidelines that are feasible to operationalize and more appropriately target populations with highest LTBI risk, as well as to identify strategies to support guideline implementation,” Ku said.
Perspective
Back to Top

David L. Cohn, MD
The study by Ku and colleagues on LTBI testing practices in a large integrated health care system (Kaiser Permanente Southern California) has the strength of using a large sample size from its comprehensive electronic health record system, i.e, over 3.8 million adults during a 12-year period, facilitating the evaluation of a number of demographic and clinical risk factors related to LTBI testing and test positivity.
The risk factors for test positivity (by tuberculin skin tests and/or interferon gamma release assay [IGRA]) were as expected, with higher odds ratios for non-U.S. born persons, patients with HBV and HCV, diabetes, smoking, etc. The overall test positivity rate of 9% is reasonable case finding for an entire health care system and very good at 22% to 25% for persons born in countries with high rates of TB. And the high rates of testing of immunocompromised patients was excellent.
On the other hand, the disconnect between the rates of positivity and the groups who were actually tested raises questions about the optimal targeting of the populations at highest risk for LTBI and TB.
The study begs the question about next steps, ie, how many of the persons with LTBI were then treated and, of those, how many completed therapy. A review and meta-analysis of the cascade of care for LTBI showed that of persons with LTBI, only 35% were recommended for treatment and 19% completed therapy.
There are many reasons for these bumps along the road beyond the scope of this perspective, but with improvements in screening of at-risk groups as suggested by the study of Ku and colleagues, along with more widespread testing with IGRAs rather than tuberculin skin tests, and the use of currently recommended 3- to 4-month, well-tolerated rifamycin-based regimens, diagnosis and treatment of LTBI as an essential TB control strategy can be markedly enhanced.
David L. Cohn, MD
Infectious Disease News Editorial Board Member
Professor of medicine, division of infectious diseases
University of Colorado School of Medicine
Disclosures: Cohn reports no relevant financial disclosures.
Published by:
![]()
Sources/Disclosures
Collapse
Disclosures:
Ku reports receiving research funding from GSK and Moderna. Please see the study for all other authors’ relevant financial disclosures.
Add topic to email alerts
Receive an email when new articles are posted on
Please provide your email address to receive an email when new articles are posted on .
”
data-action=”subscribe”>
Subscribe
We were unable to process your request. Please try again later. If you continue to have this issue please contact [email protected].
Back to Healio