Some children avoid peanuts despite negative oral food challenges
January 16, 2024
3 min read
Add topic to email alerts
Receive an email when new articles are posted on
Please provide your email address to receive an email when new articles are posted on .
”
data-action=”subscribe”>
Subscribe
We were unable to process your request. Please try again later. If you continue to have this issue please contact [email protected].
Back to Healio
Key takeaways:
- About one in 10 children avoided peanut and one in five infrequently ingested peanut after a negative oral food challenge.
- Parent-reported peanut allergy was the most common reason for avoidance.
Children from families with a history of allergic conditions may avoid peanut ingestion even after they have had negative oral food challenges, according to a study published in The Journal of Allergy and Clinical Immunology: In Practice.
Targeted strategies may encourage these families to include peanut in their diets, the researchers wrote.
Data were derived from Leong O W-Y, et al. J Allergy Clin Immunol Pract. 2023;doi:10.1016/j.jaip.2023.10.050.
“Given the paradigm shift in food allergy prevention from widespread allergen avoidance in infancy to active introduction, unnecessary allergen avoidance following a negative oral food challenge is a significant concern,” Omega Wai-Yan Leong, BMedSci, MBBS(Hons), FRACP, researcher, and Rachel L. Peters, PhD, associate professor, both of population health, Murdoch Children’s Research Institute, Australia, told Healio in a joint statement.
Study design, results
Using the population-based HealthNuts study, the researchers assessed the frequency of unnecessary allergen avoidance following negative peanut OFCs.
Also, the researchers examined whether there were any characteristics that clinicians could be mindful of to identify families who may require additional education on the importance of allergen consumption for food allergy prevention.
The study examined data from 593 children who participated in an OFC for peanut at age 1 year, including 420 whose OFCs were negative. The children with negative OFCs included 164 who had a skin prick test result of 0 mm and 233 with a SPT result of 1 mm or greater at the time of the OFC.
At age 4 years, 296 (70.5%) of the caregivers of children with negative OFCs completed a questionnaire, and 10.2% (95% CI, 6.9%-14.4%) reported that they were still actively avoiding peanut in their child’s diet.
Reasons for continuing to avoid peanut included a parent-reported peanut allergy in the child (67.9%) and a family history of food allergy (17.8%). Also, 14.3% gave their reason as “other,” which included peanuts being a choking hazard, children disliking the taste or children being fussy eaters.
The 28 children whose parents excluded peanut from their diets at age 4 years included 22 who had SPT at age 4 years. Eighteen of these children were not sensitized and considered tolerant. One was sensitized but passed an OFC.
Also, three of these children were sensitized, and an OFC confirmed late-onset peanut allergy. These three children also had positive peanut SPT at age 1 year.
Overall, 18.3% (95% CI, 13.9%-23.3%) of the children with negative peanut OFCs at age 1 year infrequently ingested peanut, defined as a range of never to less than three times. Proportions of children with infrequent ingestion were similar between children with negative or positive peanut SPTs at recruitment.
“Despite having a negative OFC and tolerating two teaspoons of peanut butter without reaction in infancy, almost one in five children were not eating peanut frequently by age 4 years,” Leong and Peters said.
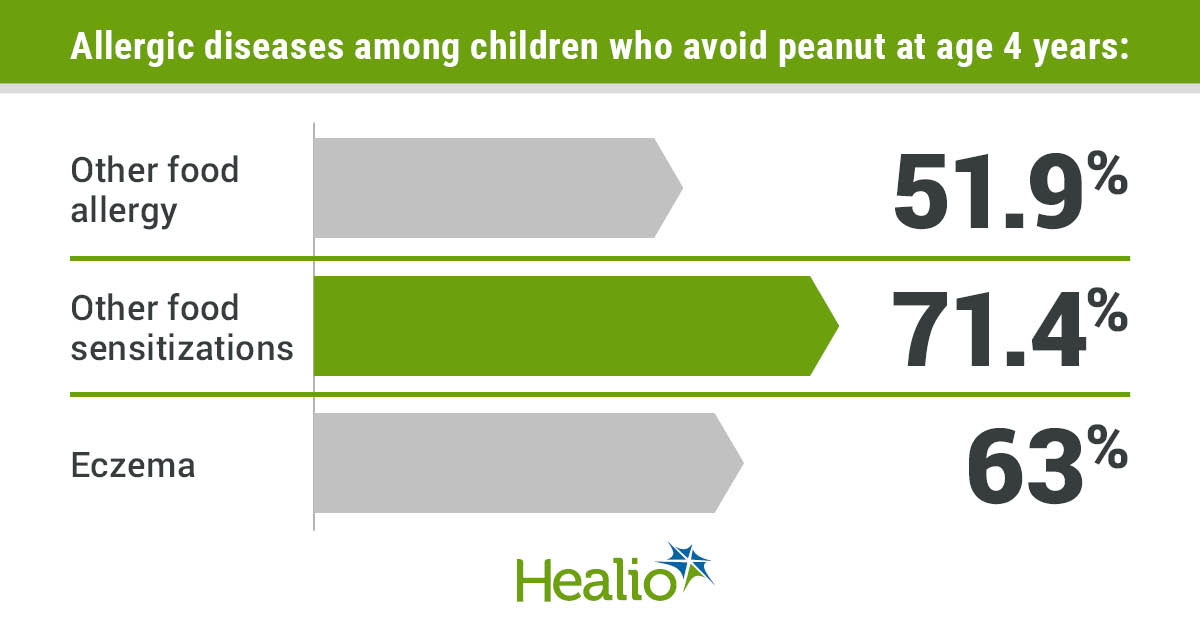
The children with a negative peanut OFC at age 1 year along with other allergic diseases were more likely to avoid peanuts at age 4 years than those who did not have other allergic diseases, the researchers said.
Specifically, children who avoided peanut included 51.9% of those who had another food allergy and 25.3% of those who did not; 71.4% of those with other food sensitizations and 35.9% of those who did not; and 63% of those who had eczema and 43.1% of those who did not.
Despite a negative OFC, the researchers continued, children were less likely to have eaten peanut more than three times if they had a sesame or egg allergy, if the family had a history of food allergy or if the caregivers believed the child was at risk for food allergy before the peanut OFC at age 1 year.
Most of the children had not eaten peanut before age 1 year, the researchers added, but the children who did were more likely to continue peanut ingestion.
Conclusions, next steps
Based on these findings, the researchers urged clinicians to identify factors associated with peanut avoidance or infrequent peanut ingestion in patients with negative OFCs and initiate interventions to encourage peanut consumption.
“Peanut avoidance in early life has been linked to the development of peanut allergy, and continued avoidance of peanut after resolution of peanut allergy has been associated with recurrence of the allergy,” Leong and Peters said.
The researchers said they were surprised that the most common reason given for not eating peanut was that the child had a peanut allergy, despite passing the OFC.
“Children who had other food allergies, or if there was family history of food allergies, were more likely to be avoiding peanut than children without a personal or family history of food allergy,” Leong and Peters said.
The researchers recommended discussing the complications that may follow peanut avoidance with these families, providing printed and online resources, sending automated reminders to include peanut in diets via email or text, follow-up telephone calls and follow-up allergy clinic visits within 3 to 6 months of a negative OFC.
“Clinicians can encourage families to incorporate peanut into the diet of infants following a negative OFC by educating families and increasing awareness of the importance of allergen ingestion to prevent food allergy,” Leong and Peters said. “Further evaluation of the effectiveness of these strategies would be useful.”
For more information:
Omega Wai-Yan Leong, BMedSci, MBBS(Hons), FRACP, can be reached at [email protected]. Rachel L. Peters, PhD, can be reached at [email protected].
Perspective
Back to Top
Sandra J. Hong, MD
Early introduction of peanuts is so important for this age group because it is one of the only things that we know that can absolutely prevent people at high risk for food allergy from developing that allergy.
The LEAP trial, which looked at babies who were at extremely high risk for developing a peanut allergy, was the first time, basically, that we realized that there is something proactively that we could do to prevent food allergies, which was huge.
These children had a history of an egg allergy and/or they had eczema. We know that those kids are going to be the ones that we would be most concerned about, and they were able to decrease that risk in about a quarter of these children. It was an exciting study.
A lot of times, the families we treat come to us after they already have had a reaction to a food, so our population is a little bit different from the one in this study, which included individuals who had not had any reaction.
However, I could see why the 10% of parents in this study had concerns and continued to avoid peanut even after having a negative challenge, as 67% of the families in this study thought they might be allergic because they had other food allergies such as cashew or tree nut.
A lot of families don’t realize that you don’t have to have a peanut allergy if you’ve got a tree nut allergy. A lot of times, individuals think that peanuts and tree nuts are all nuts, so that can be confusing. Additionally, they had eczema with other allergies, and about 20% of them had a family history of food allergies.
A lot of times, I will see families whose first child has a peanut allergy. With their next child, they’re concerned about the risks of bringing peanut into the home, which may cause the first child to have a reaction. They feel like it is the best move to just avoid peanut altogether. I would encourage these families to make sure that their second child is safely getting peanut into their diet so they don’t end up with a peanut allergy.
If there isn’t enough great communication regarding a challenge and what it means — that they aren’t showing any evidence of a peanut allergy and that they should continue to eat peanut in their diet at least three times a week — it may be confusing.
Physicians need to have a conversation with these families, telling them that their child is at increased risk for peanut allergy and that they need to include peanut in their diet. We performed the challenge and know that their child does not have a peanut allergy at this moment. But we have this window of time when it is extremely important to get peanut into the infant’s diet so the body does not think that it’s foreign and begin developing antibodies.
Looking ahead, I would be interested in these families. As a practicing allergist, I will see children with peanut allergies in addition to allergic reactions to, say, cashew. We will test and other tree nuts might come up positive. We will be able to say that they aren’t allergic to, say, walnuts.
We have to make sure that we have these conversations and tell them that we would like them to keep these other foods in their diet so they don’t develop an allergy. We have to be proactive in our wording. We should have educational handouts. Maybe we should include this information in patient portals such as MyChart. And, we should follow up later to make sure that these families continued to include these foods in their diets.
It also would be interesting to see if these interventions increased these families’ ability to eat these foods and maintain them in their diets or if, as in this study, families continued to avoid these foods.
I understand it from a family standpoint, but it does create challenges further down the line when they are teenagers or young adults and going off to college. Now they think they’re allergic to all of the tree nuts, for instance, when it’s only cashews that they really need to be worried about.
Sandra J. Hong, MD
Allergist and Director, Food Allergy Center of Excellence, Cleveland Clinic
Disclosures: Hong reports no relevant financial disclosures.
Sources/Disclosures
Collapse
Disclosures:
Leong reports no relevant financial disclosures. Peters reports receiving consultant fees from Gerson Lehrman Group. Please see the study for all other authors’ relevant financial disclosures.
Add topic to email alerts
Receive an email when new articles are posted on
Please provide your email address to receive an email when new articles are posted on .
”
data-action=”subscribe”>
Subscribe
We were unable to process your request. Please try again later. If you continue to have this issue please contact [email protected].
Back to Healio