EHR data reveal patterns in pediatric allergy development
August 04, 2023
5 min read
ADD TOPIC TO EMAIL ALERTS
Receive an email when new articles are posted on
Please provide your email address to receive an email when new articles are posted on .
”
data-action=”subscribe”>
Subscribe
We were unable to process your request. Please try again later. If you continue to have this issue please contact [email protected].
Back to Healio
Key takeaways:
- Peanut, egg and shellfish were the most common IgE-mediated food allergies.
- The atopic march often starts with atopic dermatitis in infancy.
- Asthma and allergic rhinitis were common comorbidities.
Patterns of pediatric allergy demonstrated a population-level progression of diseases in an atopic march from eczema to food allergies, asthma and environmental allergies, according to a study published in Pediatrics.
Electronic health records enabled this first-time analysis of data from disparate pediatric practices and health systems nationwide, according to Stanislaw J. Gabryszewski, MD, PhD, fellow in the division of allergy and immunology at Children’s Hospital of Philadelphia, and colleagues.
Data were derived from Gabryszewski SJ, et al. Pediatrics. 2023;doi:10.1542/peds.2022-060531.
“We were interested in studying patterns of allergy in children across the United States. This is an important area of focus because we know that when allergies are not fully treated, they can have a negative effect on children’s quality of life,” Gabryszewski told Healio.

Stanislaw J. Gabryszewski,
“To improve how clinicians can diagnose and treat allergies in children, it is important that we have an accurate understanding of how widespread they are and why some children are more likely to develop allergies over others,” he said.
Most studies of allergy patterns in children have relied on surveys completed by families, Gabryszewski said.
“Our study used a complementary approach by analyzing electronic health record information from different practices across the United States,” he said.
“This approach removes the need to survey families and expect them to remember the details about their child’s allergic condition. Ultimately, both approaches are valuable because they capture both family and clinician perspectives,” he continued.
Incidence of allergic diseases
Researchers evaluated data of 218,485 children (51.1% boys; 47.6% white; 31.9% Black; 10.2% Hispanic; 2.8% Asian or Pacific Islander) from the Comparative Effectiveness Research through Collaborative Electronic Reporting Consortium database of children born in the U.S. and observed for at least 5 years between 1999 and 2020.
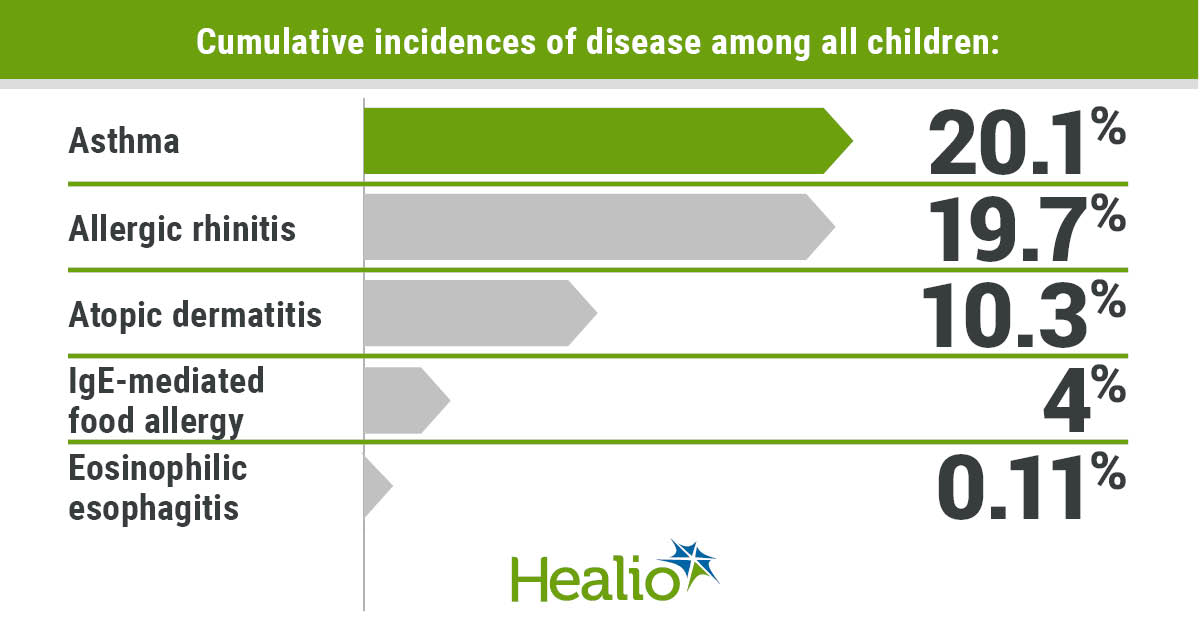
Based on diagnosis codes and medication prescriptions, researchers calculated cumulative incidences of 10.3% for atopic dermatitis, peaking at age 4 months; 4% for IgE-mediated food allergy, peaking at age 13 months; 20.1% for asthma, peaking at age 13 months; 19.7% for allergic rhinitis, peaking at age 26 months; and 0.11% for eosinophilic esophagitis, peaking at age 35 months.
Gabryszewski called the prevalence of IgE-mediated food allergy somewhat surprising.
“This type of food allergy can cause a life-threatening reaction, anaphylaxis, which needs to be treated with epinephrine,” he said. “We found that the prevalence of this food allergy was 4%. This is approximately half of the prevalence of what has been reported in previous, survey-based studies.”
Specifically for food allergies, median ages at diagnosis included age 12 months (interquartile range [IQR], 7-19) for milk, 16 months (IQR, 12-34) for egg, 18 months (IQR, 11-49) for wheat, 25 months (IQR, 15-49) for peanut, 40 months (IQR, 22-72) for fish, 52 months (IQR, 28-83) for sesame, 54 months (IQR, 30-86) for shellfish and 58 months (IQR, 34-86) for tree nuts.
During the first 5 years, cumulative incidences of food allergies were highest for peanut (1.7%), egg (0.7%) and milk (0.4%), whereas the highest cumulative incidences of food allergens overall included peanut (1.9%), egg (0.8%) and shellfish (0.6%).
Also, 37.4% of children with a food allergy were allergic to two or more distinct foods.
Comorbidities
Among the full cohort, 23.3% had one allergic manifestation, 9.9% had two, 2.8% had three, 0.6% had four and 0.01% had five.
There were marked comorbidities among children with respiratory allergies, the researchers noted, including 43.9% of patients with asthma who also had allergic rhinitis and 44.8% of patients with allergic rhinitis who also had asthma.
Similarly, 38.3% of patients with AD, 49.6% of patients with an IgE-mediated food allergy and 64.1% of patients with EoE also had asthma, whereas 39.7% of those with AD, 46.9% of those with an IgE-mediated food allergy and 54.7% of those with EoE also had allergic rhinitis.
Plus, 33.1% of the patients with an IgE-mediated food allergy also had AD, and 40.6% of those with EoE had an IgE-mediated food allergy diagnosis as well.
Gabryszewski noted that the researchers gained insight into the demographic features of patients with EoE, which does not cause anaphylaxis but does cause symptoms in the esophagus such as difficulty swallowing food.
“We found that the prevalence of EoE was about 0.1% or one in 1,000 people,” he said. “Interestingly, while previous studies suggest that this is a disease that affects mostly Caucasian males, we actually observed a higher rate of non-Caucasian children with EoE than has been previously reported, almost 40%.”
Conclusions, next steps
Calling their study unique due to its use of longitudinal data entered by primary care providers, which minimizes bias, the researchers considered their work the first to determine pediatric allergic disease patterns across multiple practices and health systems including urban, suburban and rural sites, indicating the value of EHRs as a research tool.
Also, the researchers wrote, these patterns indicate predictable sequences known as the allergic march, beginning with peak incidence of AD and consistent with the hypothesis that allergy may develop later in life after sensitization via the skin.
“As a whole, children tended to be diagnosed first with eczema, an allergic condition of the skin, followed by IgE-mediated (or anaphylactic) food allergy,” Gabryszewski said.
Allergic conditions affecting the lungs and nasal passages, asthma and allergic rhinitis, then followed, with EoE appearing last, he continued.
“Our study also describes which allergic conditions tend to occur along with other allergic conditions, such as food allergies and respiratory allergies,” he said.
These comorbidity patterns include asthma and allergic rhinitis; IgE-mediated food allergy and EoE; respiratory allergies, AD and food allergies; and EoE with all allergic conditions.
By recognizing these patterns, the researchers wrote, physicians can monitor patients for the development of additional allergies later in life.
“Our food allergy prevalence and demographic findings highlight the importance of clinicians partnering with families in diagnosing food allergies and intolerances,” Gabryszewski said.
“Additionally, they highlight the importance of continuing to do studies such as ours, so that we can accurately identify which groups of children are affected by specific allergic diseases,” he continued.
However, Gabryszewski cautioned that the allergic march does not necessarily mean that every child will develop each of these conditions.
“Rather, it helps us understand when over the course of a child’s life these conditions might appear,” he said. “Collectively, these findings are helpful for both clinicians and families, so they can be better informed about when to be on the lookout for the possible development of new allergic conditions.”
Gabryszewski also said that accurate knowledge about these patterns enables the profession to learn how widespread these diseases are and which groups of children tend to be most affected.
“There are still many unanswered questions about potential interventions that could help halt allergic progression in children,” he said. “Knowledge stemming from our study will inform how to allocate research funding which will, in turn, inform future public health and policy measures.”
Next, the researchers hope to determine why, at the individual level, some children do not develop allergies in the typical allergic march sequence.
“For example, some children only develop one allergy, while others may develop multiple allergies, but in a different sequence,” Gabryszewski said. “Identifying risk factors that can help us predict whether a child may develop one or more allergies has the potential to inform personalized medicine in the future.”
ADD TOPIC TO EMAIL ALERTS
Receive an email when new articles are posted on
Please provide your email address to receive an email when new articles are posted on .
”
data-action=”subscribe”>
Subscribe
We were unable to process your request. Please try again later. If you continue to have this issue please contact [email protected].
Back to Healio