Sleep-disordered breathing more frequently in men with vs. without HIV
Source/Disclosures
Disclosures:
Punjabi reports receiving research grant support from Philip-Respironics and ResMed for work unrelated to this manuscript. Please see the study for all other authors’ relevant financial disclosures.
ADD TOPIC TO EMAIL ALERTS
Receive an email when new articles are posted on
Please provide your email address to receive an email when new articles are posted on . ” data-action=”subscribe”> Subscribe
We were unable to process your request. Please try again later. If you continue to have this issue please contact [email protected].
Back to Healio
Key takeaways:
- Four different measures of sleep-disordered breathing were compared between men with vs. without HIV.
- Men with vs. without HIV experienced more mild and moderate sleep-disordered breathing.
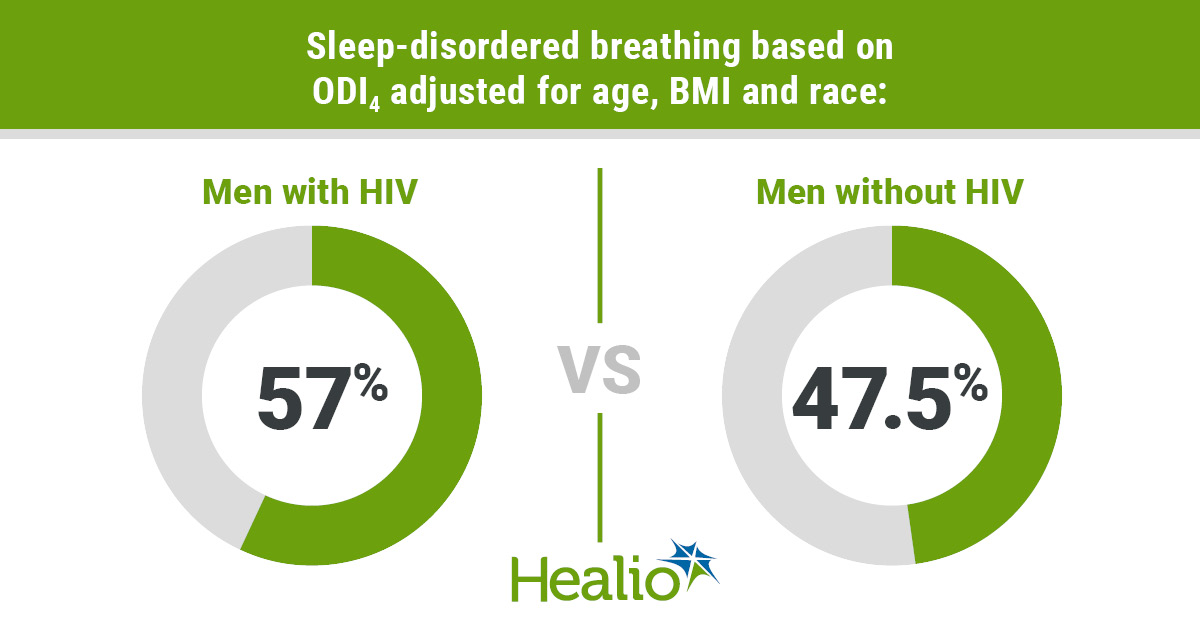
When evaluating oxygen desaturation index scores with 4% desaturation, sleep-disordered breathing was found more often in men with vs. without HIV, according to study results published in CHEST.
“The current study found that men with HIV showed a higher prevalence of sleep-disordered breathing than men without HIV, based on the 4% oxyhemoglobin desaturation threshold for defining sleep-disordered breathing-related events even after accounting for known risk factors for sleep-disordered breathing such as age, BMI and race,” Naresh M. Punjabi, MD, Ph.D, chief of the division of pulmonary, critical care and sleep medicine at the University of Miami Miller School of Medicine, and colleagues wrote.
Data were derived from Punjabi NM, et al. CHEST. 2023;doi:10.1016/j.chest.2022.10.030.
Punjabi and colleagues analyzed 466 men with HIV (mean age, 54.9 years; 57.1% white; BMI, 27.2 kg/m2) and 370 men without HIV (mean age, 60.8 years; 76.8% white; BMI, 27.9 kg/m2) from the multicenter AIDS cohort study to understand the frequency of sleep-disordered breathing and compare predictors of this condition in both sets of men.
Researchers identified sleep-disordered breathing from participants’ home polysomnography tests, in which this condition was determined by five or more events per hour on an oxygen desaturation index with a 3% (ODI3) or 4% (ODI4) threshold of oxygen desaturation or an apnea-hypopnea index with a 3% oxygen desaturation/EEG arousal (AHI3a) or 4% (AHI4) oxygen desaturation.
Using the number of events per hour, researchers identified the severity of an individual’s sleep-disordered breathing, with 5 to 14.9 events per hour demonstrating a mild condition, 15 to 29.9 events per hour demonstrating a moderate condition and 30 or more events per hour demonstrating a severe condition.
When assessing ODI3 and AHI3a between both sets of men, researchers found a comparable frequency of sleep-disordered breathing following age, BMI and race adjustments (ODI3 among men with HIV, 83% vs. men without HIV, 80.6%; AHI3a among men with HIV, 88.1% vs. men without HIV, 85.8%), but this was not true with use of ODI and AHI with 4% oxygen desaturation. When using these two measures, more men with HIV had sleep-disordered breathing compared with men without HIV (ODI4, 57% vs 47.5%; P = .04; AHI4, 58.6% vs 49.9%).
Among men who received a score of 11 or higher on the Epworth sleepiness scale, which signifies daytime sleepiness, those with HIV more frequently had sleep-disordered breathing vs. those without HIV across both ODI at 3% (17.1% vs. 11.4%) or 4% (11.2% vs. 6.4%) desaturation, as well as AHI at 3% (17.5% vs. 13.2%) or 4% desaturation (11. 8% vs. 7.1%), according to researchers.
Notably, the odds for sleep-disordered breathing among those with daytime sleepiness were greater when using 4% desaturation (ODI4, adjusted OR = 1.83; 95% CI, 1.12-2.99; AHI4, aOR = 1.74; 95% CI, 1.09-2.77).
Researchers also found that men with HIV experienced more mild and moderate sleep-disordered breathing vs. men without HIV when using ODI4 (mild aOR = 1.46; 95% CI, 1.03-2.07; moderate aOR = 1.84; 95% CI, 1.15-2.95). The same result occurred with AHI4 (mild aOR = 1.45; 95% CI, 1.02-2.06; moderate aOR = 1.67; 95% CI, 1.04-2.67).
Among both sets of men, age, race and BMI were linked to sleep-disordered breathing; however, researchers observed three factors not related to the condition in men with HIV, including viral load, CD4 cell count and antiretroviral medication use.
“Although the pathophysiologic basis of sleep-disordered breathing in people with HIV needs further study, the clinical impact of sleep-disordered breathing is known,” Punjabi and colleagues wrote.
“Considering the effects of sleep-disordered breathing on sleepiness and quality of life, case identification of sleep-disordered breathing in people with HIV whose disease remains undiagnosed is of clinical value given the associated improvements with positive airway pressure therapy,” Punjabi and colleagues added. “Conventional strategies used for diagnosing sleep-disordered breathing with portable home testing can be used in people with HIV because there is no evidence that diagnostic accuracy of such approaches varies as a function of HIV status.”
perspective
back to top

Nilong Vyas, MD
The prevalence of sleep disordered breathing (SDB) is approximately 50% in the average male patient. This study looked at the prevalence of SDB in men with and without HIV. The results found that SDB prevalence is high overall among the men tested; however, it is more prevalent in those with HIV than without HIV when using the ODI4 scale of measurement, which is the oxygen desaturation index where at least 4% desaturation occurred.
The findings that there is an increased prevalence of SDB in patients with HIV are not surprising because it is possible that the decreased diffusing capacity of the lung in people with HIV may possibly contribute to increased desaturation episodes leading to worsening hypoxemia and more SDB episodes during sleep.
More research needs to be conducted specifically into HIV-induced lung dysfunction vs. physiologic upper airway collapse that occurs during sleep in those patients with and without SDB.
It is important for there to be a multidisciplinary approach to the care of a patient with HIV in order for parameters to be accounted for, including sleep hygiene and symptoms of SDB, so proper guidance can be sought. If a patient with HIV is experiencing increased daytime sleepiness and difficulty with arousal in the morning, the topic of SDB needs to be broached with their physician provider.
Nilong Vyas, MD
Pediatrician, Sleep Consultant for Sleepless in NOLA and Medical Review Expert at Sleep Foundation
Disclosures: Vyas reports no relevant financial disclosures.
ADD TOPIC TO EMAIL ALERTS
Receive an email when new articles are posted on
Please provide your email address to receive an email when new articles are posted on . ” data-action=”subscribe”> Subscribe
We were unable to process your request. Please try again later. If you continue to have this issue please contact [email protected].
Back to Healio